
Pre Exam Course Pediatric Viva
Presentation
•
Specialty
•
University
•
Medium

Ali Muhdi
Used 7+ times
FREE Resource
33 Slides • 13 Questions
1
PRE EXAM COURSE PEDIATRIC VIVA
Desember 2025
By. Dr. dr. Udi Heru Nefihancoro, Sp.B., Sp.OT.Subsp.A(K)
2
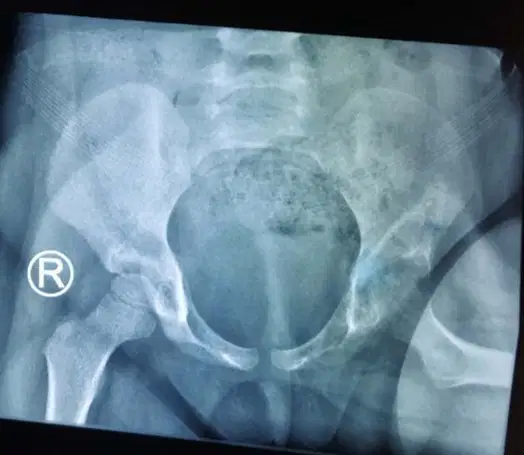
CASE 1
Girl, 6 year old
Chief complain : Unequal lower limb
Her parents noticed when patient walked, she had limping gait
No pain
No history of trauma
Patient had breech presentation delivery, without any abnormal condition in post natal care.
3
Multiple Choice

What is your diagnosis ?
Old dislocation of right Hip
Proximal Femur Focal Deficiency
Residual effects of Hip infective arthritis
Developmental Dysplasia of Right Hip
Right Femoral Neck fracture
4
ANSWER
"Developmental dysplasia of the hip"
Occurs due to an abnormal hip development, presenting in infancy or early childhood with a spectrum ranging from dysplasia to dislocation of the hip joint.
Developmental dysplasia of the hip encompasses several hip abnormalities, including instability, acetabular dysplasia, subluxation, and dislocation.

6
ANSWER
"Breech position":
In the last trimester, breech position is the most significant risk factor for developmental dysplasia of the hip, with an odds ratio of 5.47 (2.58 to 11.6).
Procedures that decrease the time spent in the breech position (eg. external cephalic version and prelabor cesarean section) reduce the risk for developmental dysplasia of the hip.
7
Multiple Choice

What is clinical examination should be performed in Newborn Screening ?
Ortolani manuver
Barlow manuver
Klissic tes
All of Them
Ortolani maneuver & Barlow maneuver
8
ANSWER
Newborn Screening
Ortolani maneuver:
With the infant in the supine position, the hip is flexed at 90° and in neutral rotation. The infant should be calm with clothes and diapers removed. This maneuver aims to reduce the dislocated hip by holding the hip so that the thumb is on the inner aspect and the index and ring finger are on the greater trochanter. While applying anterior force on the greater trochanter, gently abduct the hip. Clinicians will feel a jerk or clunk if the hip is dislocated. However, "hip clicks" are clinically insignificant without instability.
Barlow maneuver:
Employing the same initial position as the Ortolani maneuver, force may be applied posteriorly to the trochanter, although the AAP recommends against posterior force, and the hip is adducted.
A clunk or jerk is felt if the hip can be dislocated. This maneuver should be performed gently, as forceful adduction can cause instability.

10
Explanation
4. PATIENT PREPARATION IN OT
This scenario is an open technique of Anterior Hip approach
We will setup involves positioning of the patient supine on an operating table.

11
Explanation

5. Anterior approach to the pediatric proximal femur
Preliminary remarks
The anterior approach provides the most direct access to the anterior aspect of the hip. Many surgeons prefer this approach for reduction of femoral head and neck fractures.
Note: Fixation of femoral neck fractures reduced through this approach will require separate percutaneous screw insertion, or a separate lateral incision.
12
Vascular anatomy
The deep branch of the medial femoral circumflex artery provides the main relevant blood supply to the femoral head.
The medial femoral circumflex artery originates from the deep femoral artery (profunda femoris), courses between the iliopsoas and pectineus muscles, and runs posteriorly between the femur and the pelvis.
During its course, a small branch supplies the inferior retinaculum (ligament of Weitbrecht).
The main branch of the medial femoral circumflex artery is related to the inferior border of the obturator externus muscle and passes posterior to the femur, towards the intertrochanteric crest.
It then crosses posterior to the obturator externus and anterior to the triceps coxae (obturator internus and the superior and inferior gemelli).
Before crossing the triceps coxae, a small branch passes to the greater trochanter.
The vessel enters the joint capsule between the gemellus superior and the piriformis muscles.
Note: The approach must always be cranial to the piriformis muscle. This anatomical detail is crucial when starting to prepare the capsule.
After perforating the capsule, the vessel passes along the superior retinaculum and splits into 3-4 branches. Provided the obturator externus muscle remains intact, it will protect the medial femoral circumflex artery.

13
Skin incision
Superficial dissection

A bikini incision is used. The level of the incision is below the anterior superior iliac spine and centered on the anterior inferior iliac spine.
After incision of the skin and fat, the deep fascia is encountered.
The interval between tensor fascia lata and sartorius is identified by palpation and the fascia incised.
14
Deep dissection
The fascia should be carefully incised and the lateral cutaneous nerve of the thigh identified and protected.
Note:
Dissection within the medial edge of tensor fascia lata is preferred by some surgeons and helps to protect the lateral cutaneous nerve of the thigh.

15

16
CASE 2
Boy 6 y.o
Chief complain : Severe pain in right elbow
After fell-down from kindergarten monkey bar, 1 hour ago
Accompanied by his mother and teacher
Hematoma on anterior part of right elbow, no bruise
Normal pulse of radial artery
Numbness on 2nd & 3rd fingers

17

18
Multiple Choice

WHAT IS YOUR DIAGNOSIS ?
CLOSED FRACTURE LATERAL CONDYLE HUMERUS WITH MEDIAN NERVE INJURY
CLOSED FRACTURE LATERAL CONDYLE HUMERUS WITH RADIAL NERVE INJURY
CLOSED FRACTURE MEDIAL CONDYLE HUMERUS WITH MEDIAN NERVE INJURY
19
CASE 2
1. WHAT IS YOUR DIAGNOSIS ?
CLOSED SUPRACONDYLAR FRACTURE WITH MEDIAN NERVE INJURY

20
Multiple Choice

WHAT IS PUCKER SIGN ?
Skin discoloration caused by hematoma formation
Soft tissue defect from proximal fragment penetration into subcutaneous tissue, indicating significant soft tissue injury and possible median nerve/brachial artery entrapment
Swelling of the soft tissue distal to the fracture
Dimpling of the skin due to severe edema
21
CASE 2
2. WHAT IS PUCKER SIGN ?
A soft tissue defect ( proximal fracture fragment penetration through the brachialis muscle and anterior fascia into subcutaneous tissue ) and is indicative of significant soft tissue injury from an extension-type fracture with potential entrapment of median nerve and brachial artery

22
Multiple Choice

WHAT CLASSIFICATION OF THIS TYPE FRACTURE
Salter-Harris Type II
Gartland Extension Type II
Gartland Extension Type III
Gustilo-Anderson Type II
23
CASE 2
3. WHAT CLASSIFICATION OF THIS TYPE FRACTURE
GARTLAND EXTENSION TYPE 3

24
Multiple Choice
WHAT WILL YOU DO ? HOW TO MANAGED THE FRACTURE ?
OPEN REDUCTION & EXPLORATION
PUT ON SPLINT
OBSERVATION
25
CASE 2
4. WHAT WILL YOU DO ? HOW TO MANAGED THE FRACTURE ?
PUT ON SPLINT, RECHECK THE NUMBNESS IF STILL PRESENT, WE PLAN TO DO OPEN REDUCTION & EXPLORATION
26
Multiple Choice
EXPLAIN YOUR SURGICAL TECHNIQUE PLAN
This scenario is an open technique of posterior approach.
This scenario is an open technique of lateral approach.
This scenario is an open technique of anterior approach.
This scenario is an open technique of medial approach.
27
CASE 2
5. EXPLAIN YOUR SURGICAL TECHNIQUE PLAN
This scenario is an open technique of anterior approach.
The setup involves positioning of the patient supine on an operating table with a radiolucent hand table attached
Anterior Approach, indications :
Irreducible extension-type fractures
Suspected interposition brachialis muscle and fascia
Median nerve sensory deficits
Vascular exploration
The anterior approach provides direct access to interposed soft tissue in irreducible extension-type fractures. can also be extended to facilitate neurovascular repair when necessary.

28
Anterior Approach

29
Anterior Approach

30
CASE 3
Girl, 4 year old
Chief complaint : Pain of the left hip
The patient felt pain on the left hip since 3 months ago and worsen since 1 month ago. She couldn’t walk anymore.
There was history of cough, fever, decrease of weight, decrease of appetite, and night sweating. Patient has consumed Anti TB drugs since 1 month ago
31
CASE 3

32
Multiple Choice
What is your most possible diagnosis ?
Avascular Necrosis
Coxitis TB
Chondro sarcoma
SCFE
Not all of them
33
CASE 3

34
Multiple Choice
What treatment do you suggest ?
Effective chemotherapy
Skeletal traction
Synovectomy and joint debridement
Effective chemotherapy, synovectomy and joint debridement
Not all of them
35
Development of interval between tensor fascia lata and sartorius

36

37

38
CASE 4
Male
13 year old
Chief complain : Unable to straightened and bent maximally on right elbow
Patient had history of fell down from tree
39
CASE 4
40
CASE 4
X-Ray Right Elbow AP/ Lat

41
CASE 4
CT-Scan Right Elbow AP/ Lat

42
Multiple Choice
What is the diagnosis ?
Malunion supracondylar humerus fracture
Malunion lateral condylar humerus fracture
Malunion medial epicondyle humerus fracture
None
43
1. WHAT IS THE DIAGNOSIS?
Malunion medial epicondyle humerus fracture
44
Multiple Choice
What treatment do you suggest ?
POSTERIOR WEDGE SUPRACONDYLAR OSTEOTOMY
LATERAL WEDGE SUPRACONDYLAR OSTEOTOMY
MEDIAL WEDGE SUPRACONDYLAR OSTEOTOMY
ANTERIOR WEDGE SUPRACONDYLAR OSTEOTOMY
45
2. WHAT TREATMENT DO YOU SUGGEST?
ANTERIOR WEDGE SUPRACONDYLAR OSTEOTOMY
Since the patient is right-handed, they should be able to bring food to their mouth with their right hand. Therefore, we should consider adding elbow flexion, as opposed to extension

46

THANK YOU
PRE EXAM COURSE PEDIATRIC VIVA
Desember 2025
By. Dr. dr. Udi Heru Nefihancoro, Sp.B., Sp.OT.Subsp.A(K)
Show answer
Auto Play
Slide 1 / 46
SLIDE
Similar Resources on Wayground

44 questions
Apps & applications
Presentation
•
Professional Development
41 questions
Problem- Solving
Presentation
•
KG
42 questions
Chapter 5: Sexual Orientation
Presentation
•
University
40 questions
Kingdoms
Presentation
•
KG - University
42 questions
Storytelling and Narrative
Presentation
•
University
41 questions
Магистранты. К.р.№1
Presentation
•
University
43 questions
BBB3013 Noun (N) / Noun Phrase (NP)
Presentation
•
University
39 questions
Articles 101
Presentation
•
University
Popular Resources on Wayground
19 questions
Naming Polygons
Quiz
•
3rd Grade
10 questions
Prime Factorization
Quiz
•
6th Grade
20 questions
Math Review
Quiz
•
3rd Grade
15 questions
Fast food
Quiz
•
7th Grade
20 questions
Main Idea and Details
Quiz
•
5th Grade
20 questions
Context Clues
Quiz
•
6th Grade
20 questions
Inferences
Quiz
•
4th Grade
19 questions
Classifying Quadrilaterals
Quiz
•
3rd Grade
Discover more resources for Specialty
50 questions
ELA EOG Prep 7th Grade
Quiz
•
KG - University
20 questions
Guess The App
Quiz
•
KG - Professional Dev...
11 questions
dog breeds
Quiz
•
3rd Grade - Professio...
11 questions
NFL Football logos
Quiz
•
KG - Professional Dev...
19 questions
Minecraft
Quiz
•
6th Grade - Professio...
20 questions
Block Buster Movies
Quiz
•
10th Grade - Professi...
10 questions
Would you rather...
Quiz
•
KG - University
49 questions
AP Environmental Science Final Exam Review
Quiz
•
10th Grade - University