
Endocrinology
Presentation
•
Biology
•
Professional Development
•
Hard
Standards-aligned

MD undefined
Used 5+ times
FREE Resource
26 Slides • 23 Questions
1
Endocrinology Board Review
By MS
2
Multiple Choice
Most common cause of subclinical hyperthyroidism
Toxic multinodular goiter
Graves’ Disease
Subacute Thyroiditis
TSH-secreting pituitary adenoma
3
Multiple Choice

A 40-year-old woman with recently diagnosed primary hyperparathyroidism is evaluated with an abdominal radiograph.
Which of the following is the most likely diagnosis?
Chronic pancreatitis
Nephrocalcinosis
Nephrolithiasis
Renal cell carcinoma
4
Nephrocalcinosis is calcium deposition in renal parenchyma- Mechanism: Excess PTH drives hypercalcemia and hypercalciuria, promoting calcium-phosphate deposition in tubules and interstitium
Imaging: Ultrasound shows echogenic foci; CT/MRI define extent and guide management .
Biochemistry: Elevated calcium, PTH, and 24-hour urine calcium > 400 mg/d support the diagnosis
Complications: AKI, nephrolithiasis, and chronic kidney disease are common
Management: Parathyroidectomy is definitive; hydration and bisphosphonates are adjuncts
5
Multiple Choice

A 43-year-old man has developed changes in skin color and is evaluated for weight loss, nausea, and weakness.
Skin findings are shown.
Which of the following is the most likely diagnosis?
Acanthosis nigricans
Diffuse melanosis cutis
Primary adrenal insufficiency
Secondary adrenal insufficiency
6
Primary adrenal insufficiency.
Physical examination is helpful in the differentiation of primary (adrenal) from secondary (pituitary) causes of adrenal insufficiency;
Only patients with primary adrenal insufficiency have excessive adrenocorticotropic hormone, melanocyte-stimulating hormone, and pro-opiomelanocortin secretion, which results in darkly pigmented skin
7
Multiple Choice
An 81-year-old man is evaluated for a 3-month history of fatigue, constipation, cognitive symptoms, and cold intolerance. He has gained 4.5 kg (10 lb) during the past year. Medical history is significant for CAD. Medications are rosuvastatin, lisinopril, metoprolol, and aspirin.
On physical examination, pulse rate is 54/min. Weight is 65 kg (143.0 lb). The thyroid is firm but not enlarged, the skin is cool and dry, and his hair is coarse. Deep tendon reflexes are delayed.
Laboratory studies show a thyroid-stimulating hormone level of 25 µU/mL and free thyroxine level of 0.5 ng/dL (0.9-1.4)
Most appropriate treatment?
Levothyroxine, 25 μg/d
Levothyroxine, 100 μg/d
Thyroid, desiccated, 60 mg/d
Triiodothyronine, 50 μg/d
8
Treatment: Levothyroxine is first‑line for hypothyroidism
Dose: Full replacement ≈ 1.6 μg/kg (lean body weight)
Exceptions: Start low (25–50 μg/day) in older adults or CAD
Rationale: Thyroid hormone ↑ cardiac demand → risk of angina
9
Multiple Choice

A 40-year-old woman with symptoms of hyperthyroidism and a suppressed thyroid-stimulating hormone level is evaluated for a left thyroid nodule. Thyroid scintigraphy is performed.
Dx?
Autonomously functioning thyroid adenoma
Graves disease
Multinodular goiter
Thyroid cancer
10
Diagnosis: Autonomously functioning thyroid adenoma (toxic nodule)
Key labs: Suppressed TSH
Next test: Thyroid scintigraphy
Finding: “Hot” nodule with increased radioactive iodine uptake
Management: Usually benign → no biopsy needed
Ex: "cold" nodule is below

11
Multiple Choice
A 55-year-old man is evaluated for a 1-year history of decreased libido, erectile dysfunction, and fatigue. Medical history is also significant for opioid use disorder treated with methadone. He takes no other medications. On physical examination, vital signs are normal. BMI is 25. The remainder of the examination, including genital and prostate examination, is normal. A morning testosterone level obtained 4 weeks ago is low. Pituitary MRI is normal.
Laboratory studies:
Hemoglobin Normal
Follicle-stimulating hormone 2.1 mU/mL (5-15)
Luteinizing hormone 1.4 mU/mL (3-15)
Prolactin 18 ng/mL (<15)
Testosterone, total (8 AM) (second measurement) 140 ng/dL (300-1200)
Which of the following is the most appropriate treatment?
Alprostadil
Cabergoline
Sildenafil
Testosterone
12
Chronic opioids leads to ↓ GnRH → ↓ LH/FSH → secondary hypogonadism
Additional: Opioids may ↑ prolactin → further GnRH suppression
Clinical:
Men: ↓ libido, ED, fatigue, low testosterone with low/normal LH/FSH
Women: Menstrual irregularities
Management:
Stop opioids if possible
If not → testosterone replacement in symptomatic men
Why not others:
Alprostadil / PDE‑5 inhibitors: improve erections only
Cabergoline(D2 agonist): unlikely to reverse opioid‑induced hypogonadism
13
Multiple Choice
A 52-year-old man with type 2 diabetes mellitus is evaluated after hospitalization for a non-ST-elevation myocardial infarction. He is currently asymptomatic. Medications are metformin, aspirin, ticagrelor, atorvastatin, metoprolol, and lisinopril.
On physical examination, vital signs are normal. BMI is 28. The general physical examination is normal.
Laboratory studies show a hemoglobin A1c level of 7.0%.
Which of the following is the most appropriate treatment?
Empagliflozin
Pramlintide
Sitagliptin
No changes in medications
14
Key Point
Among patients with type 2 diabetes mellitus who have established atherosclerotic cardiovascular disease or established kidney disease, a sodium-glucose cotransporter 2 inhibitor or glucagon-like peptide 1 receptor agonist with demonstrated cardiovascular disease benefit is recommended as part of the glucose-lowering regimen.
15
Multiple Choice
A 61-year-old woman is evaluated after an abdominal CT scan for diverticulitis revealed an incidental adrenal mass. She has no other medical problems and takes no medications.
On physical examination, vital signs are normal. The remainder of the examination is unremarkable.
Abdominal CT scan shows a 3.5-cm homogeneous left adrenal mass with a density of 13 Hounsfield units. The remainder of the scan is normal.
Serum creatinine and electrolytes are normal. Testing for mild autonomous cortisol secretion is negative.
Which of the following is the most appropriate next step in management?
Adrenal biopsy
Adrenalectomy
Screening for primary aldosteronism
Screening for pheochromocytoma
16
Key Points
In patients with incidentally noted adrenal masses, screening for pheochromocytoma is indicated if the unenhanced CT attenuation is greater than 10 Hounsfield units.
In patients with an adrenal mass, screening for primary hyperaldosteronism is indicated in the presence of hypertension or hypokalemia.

17
Multiple Choice
A 38-year-old-woman is evaluated for a 9-month history of oligomenorrhea, a deepening voice, and increased body hair. Her last menses was 3 months ago. Medical history is otherwise unremarkable, and she takes no medications.
On physical examination, vital signs are normal. She has frontal hair loss and coarse dark hairs on her chin and chest. Larynx appears larger than normal. Clitoromegaly is present on pelvic examination.
Laboratory studies show a negative pregnancy test, a dehydroepiandrosterone sulfate level of 910 μg/dL (24.7 μmol/L), and a total testosterone level of 97 ng/dL (3.4 nmol/L).
Which of the following is the most appropriate diagnostic test to perform next?
Abdominal CT
Adrenal vein sampling
Ovarian vein sampling
Pelvic ultrasonography
Pituitary MRI
18
New hyperandrogenism (premenopausal): Evaluate ovarian + adrenal sources
Key lab: Markedly ↑ DHEAS with mild ↑ testosterone → adrenal source
Threshold: DHEAS >700 μg/dL → abdominal CT next
Rationale: Adrenal androgen‑secreting tumors cause virilization and are CT‑visible
PCOS: oligomenorrhea, hirsutism, and acne,
but no deepening voice, clitoromegaly, frontal hair loss
19
Multiple Choice
A 73-year-old woman is evaluated in the emergency department after 2 days of weakness, headache, and nausea. She underwent uncomplicated transsphenoidal resection of a pituitary macroadenoma 6 days ago and was discharged from the hospital 3 days ago.
On physical examination, vital signs are normal. No orthostasis and no neurologic or visual deficits are present. Her mucous membranes are moist.
Laboratory studies show a serum sodium level of 128 mEq/L (35–145 mEq/L], TSH of 0.9 μU/mL ( 0.4–4.0 μU/mL], and free thyroxine level of 1.1 ng/dL( 0.8–1.8 ng/dL]. Before discharge, her 8 AM serum cortisol level was 15 μg/dL ( 5–25 μg/dL], and a random serum cortisol level at 3 PM was 10 μg/dL( 3–15 μg/dL].
Adrenal insufficiency
Dehydration
Secondary hypothyroidism
SIADH
20
Diagnosis: SIADH after recent pituitary surgery
Timing: Occurs 4–12 days postop (peak 7–8 days)
Mechanism: Excess ADH release from posterior pituitary manipulation
Pattern: May be part of triphasic response (DI → SIADH → permanent DI)
Management: Fluid restriction; severe cases → hypertonic saline or vaptans
Disposition: Admit if symptomatic or Na <130 mEq/L
Why not others: Cortisol, volume status, and thyroid function are normal
21
Multiple Choice
A 32-year-old woman is evaluated in the first trimester of pregnancy for a 2-week history of heat intolerance, palpitations, and tremulousness. Her only medication is folic acid.
On physical examination, pulse rate is 110/min; remaining vital signs are normal. The thyroid is nontender and symmetrically and diffusely enlarged. A fine tremor on the patient's outstretched hands is noted.
Laboratory studies show a thyroid-stimulating hormone level of less than 0.01 μU/mL (0.4–4.0 μU/mL) and free thyroxine level of 5.3 ng/dL (0.8–1.8 ng/dL).
Which of the following is the most appropriate diagnostic test?
Thyroid scintigraphy with radioactive iodine uptake
Thyroid-stimulating immunoglobulin measurement
Thyroid ultrasonography
Total triiodothyronine measurement
22
Diagnosis: Hyperthyroidism (↓ TSH, ↑ free T4/T3)
Best next test: TSI or TRAb to evaluate for Graves disease
Rationale: RAIU confirms cause but is contraindicated in pregnancy
Alternatives:
hCG‑mediated hyperthyroidism or thyroiditis → often transient
Not helpful:
Thyroid US alone (nonspecific for cause)
Total T3 (already elevated free T4; altered in pregnancy)
23
Multiple Choice
A 28-year-old woman is evaluated for a 6-month history of amenorrhea. Medical history is significant for schizophrenia. Her only medication is risperidone.
On physical examination, vital signs are normal. BMI is 28. No breast discharge is evident.
Laboratory studies:
Estradiol
10 pg/mL (50–100 pg/mL)
Follicle-stimulating hormone
1 mU/mL (5–50 mU/mL)
Prolactin
150 ng/mL (10–0 ng/mL)
Thyroid-stimulating hormone
2.2 μU/mL (0.4–4.0 μU/mL)
Thyroxine, free
1.2 ng/dL (0.8–1.8 ng/dL)
MRI reveals a normal pituitary gland.
Consultation with the patient's psychiatrist confirms that risperidone cannot be discontinued.
Which of the following is the most appropriate management?
Begin cabergoline
Begin estrogen-progesteron replacement therapy
Repeat pituitary MRI in 6 months
Repeat prolactin measurement in 6 months
24
Risperidone‑induced hyperprolactinemia → estrogen deficiency
Symptoms: Amenorrhea ± galactorrhea; risk of bone loss
Best management: Estrogen–progesterone replacement therapy
Why: Prevents long‑term sequelae of hypoestrogenism while risperidone continues
Avoid: Dopamine agonists (eg, cabergoline) → risk of psychosis
Not appropriate: Repeat MRI or watchful waiting without hormone replacement
25
Multiple Choice
A 30-year-old woman is evaluated for a 2-month history of anorexia, insomnia, palpitations, diarrhea, and an 11-kg (24.0-lb) weight loss. She reports no neck pain. She has been well otherwise and takes no medications.
On physical examination, temperature is 37.9 °C (100.0 °F), blood pressure is 118/78 mm Hg, and pulse rate is 101/min. BMI is 18. The thyroid is firm and not enlarged, with the left lobe larger than the right. No proptosis, thyroid nodules, or adenopathy are noted, and no thyroid tenderness is present.
Laboratory studies:
Thyroid-stimulating hormone
0.02 μU/mL (0.4–4.0 μU/mL)
Thyroxine, free
2.8 ng/dL (0.8–1.8 ng/dL)
Erythrocyte sedimentation rate
53 mm/h (<20 mm/h)
Human chorionic gonadotrophin: Negative
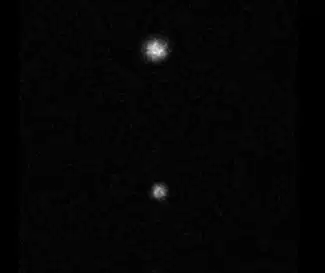
The radioactive iodine uptake scan is shown. Uptake at 24 hours is 0.3%. Which of the following is the most appropriate treatment?
Atenolol
Methimazole
Prednisone
Propylthiouracil
26
Presentation: Thyrotoxicosis (↓ TSH, ↑ free T4)
RAIU: Low uptake → destructive thyroiditis, not Graves
Supporting clues: No proptosis, ↑ ESR
Pathophysiology: Release of preformed thyroid hormone
Management: β‑blocker (atenolol) for adrenergic symptoms
Not indicated: Methimazole/PTU (no excess hormone production), prednisone (no thyroid pain)
27
Multiple Choice
A 39-year-old woman is evaluated for high-risk metastatic papillary carcinoma. She had a total thyroidectomy and iodine 131 ablation therapy 6 months ago. She is now taking levothyroxine. She is asymptomatic.
On physical examination, vital signs are normal. She has a well-healed thyroidectomy scar. There are no palpable neck masses, no adenopathy, and no tremor.
Laboratory studies:
Thyroid-stimulating hormone
0.02 μU/mL (0.5–5.0 mU/L)
Thyroxine, free
1.5 ng/dL (0.8–1.8 ng/dL)
Thyroglobulin: Absent
Antithyroglobulin antibodies: Negative
Neck ultrasound is normal.
Which of the following is the most appropriate management?
Decrease levothyroxine
Discontinue levothyroxine
Thyroid scintigraphy with radioactive iodine uptake
No change in treatment
28
Papillary thyroid cancer:
Primary treatment: Surgical resection is the cornerstone of thyroid cancer management
Adjuvant therapy: Radioactive iodine for high‑risk differentiated thyroid cancer
Long‑term management: TSH suppression with levothyroxine in high‑risk patients
After Tx, serum thyroglobulin (Tg), a sensitive marker for the detection of persistent or recurrent disease, and thyroglobulin antibody (TgAb) titers are monitored
29
Multiple Select
A 58-year-old woman presents with 1 week of palpitations and dyspnea after a similar self-limited episode 3 weeks earlier with a negative CT angiogram. She takes no medications.
Vitals show BP 150/80 mm Hg and an irregularly irregular pulse of 102/min; oxygen saturation is 95%. Exam is notable for atrial fibrillation and a large multinodular goiter.
Labs reveal suppressed TSH (<0.01 μU/mL) with elevated free T4 and total T3. ECG confirms atrial fibrillation.
Which of the following is the most appropriate initial step in management? (Choose 2)
Amiodarone
Methimazole
CT neck w/w out contrast
Propranolol
Radioactive iodine
30
Iodine‑induced hyperthyroidism (Jod‑Basedow phenomenon) after iodinated contrast in multinodular goiter
Timing: Thyrotoxicosis occurs 1–2 weeks after iodine exposure
Management: Methimazole to block thyroid hormone synthesis + propranolol for symptom control
Prevention: Avoid iodinated contrast and other iodine sources (amiodarone) when possible in multinodular goiter
31
Multiple Choice
An 83-year-old asymptomatic woman is found to have low TSH on AWE. History includes chronic stable angina and osteoporosis; she takes metoprolol, lisinopril, simvastatin, aspirin, vitamin D3, and alendronate.
Vitals are normal. The exam shows a firm, enlarged thyroid with right-sided predominance.
Subsequent labs reveal persistently suppressed TSH 0.05 μU/mL (multiple eval) with normal free T4 and total T3. Thyroid scan is provided, and 24-hour radioactive iodine uptake is 22%.
Which of the following is the most appropriate management?
Repeat thyroid-stimulating hormone test in 6 weeks
Start methimazole
Start prednisone
Start teprotumumab
32
Diagnosis: Subclinical hyperthyroidism from toxic multinodular goiter (TSH < 0.1, normal T4/T3)
Risk: Increased atrial fibrillation, CV events, bone loss with persistent TSH suppression
Best management: Start methimazole to normalize thyroid function
Why not observe: TSH suppressed for 8 weeks (TSH<0.1), with high cardiac risk
Not indicated: Prednisone (no thyroiditis), teprotumumab (no Graves/ophthalmopathy)
33
Multiple Choice
A 56-year-old hospitalized man is evaluated for abnormal thyroid tests one week after admission for E. coli urosepsis. He is receiving IV fluids, norepinephrine, and ceftriaxone.
Vitals show hypotension and tachycardia; exam reveals cool, dry skin without goiter or proptosis. TSH is low (0.11 μU/L) with mildly decreased free T4 (0.8 ng/dL). Which of the following is the most appropriate management?
Initiate levothyroxine
Initiate methimazole
Pituitary MRI
Thyroid testing after recovery
34
Key point: Avoid routine thyroid testing in hospitalized/critically ill patients
Diagnosis: Nonthyroidal illness syndrome (NTIS) (75% of hospitalized)
Typical labs: Low or low‑normal TSH, normal/low free T4, low T3, high reverse T3 (inactive form)
Mechanism: Adaptive response to illness; dopamine also can further suppress TSH
Management: No treatment; recheck TSH in ≈6 weeks after recovery
Not indicated now: Levothyroxine, methimazole, or pituitary MRI
35
Multiple Choice
A 55-year-old man reports recurrent neuroglycopenic symptoms over the past month, including a fingerstick glucose of 46 mg/dL during one episode, with relief after eating. He takes no medications.
Exam and vitals are normal; BMI is 33. Random glucose is 78 mg/dL, hemoglobin A1c is 4.7%, and other labs are normal.
Which of the following is the most appropriate diagnostic test?
72-Hour fast
Mixed meal test
Oral glucose tolerance test
Pancreatic imaging study
36
Fasting hypoglycemia: Rare without diabetes → requires evaluation
Causes: Medications, alcohol, renal/hepatic failure, adrenal insufficiency, malnutrition, prior Roux‑en‑Y gastric bypass, insulinoma (rare)
Best test: 72-hour supervised fast with insulin, C-peptide, proinsulin, and β-hydroxybutyrate at hypoglycemia
Indications: Document Whipple's triad or glucose ≤ 45 mg/dL with neuroglycopenia
Exclude: Medications, alcohol, liver/renal disease, adrenal insufficiency, malnutrition, prior bariatric surgery
Imaging: Only after biochemical confirmation of endogenous hyperinsulinism
Not indicated: Mixed meal test (postprandial), OGTT (diabetes), or imaging before biochemical proof
37
Multiple Choice
A 73-year-old woman on amiodarone for atrial fibrillation presents with recurrent AF after 1 year of therapy. She has no other medical issues or iodine exposure.
Exam shows an irregular tachycardia without thyroid abnormalities. Labs reveal suppressed TSH (<0.01 μU/mL) and elevated free T4 (3.5 ng/dL); ECG confirms atrial fibrillation. Which of the following is the most appropriate diagnostic test?
Serum thyroglobulin measurement
Thyroid peroxidase antibody titer
Thyroid scintigraphy with radioactive iodine uptake
Thyroid ultrasonography with Doppler studies
38
Thyrotoxicosis in a patient on amiodarone
Best next test: Thyroid ultrasound with Doppler
Purpose: Distinguish AIT types
Type 1 AIT → ↑ vascularity (iodine‑induced hyperthyroidism in Graves disease or thyroid nodules) Tx: methimazole
Type 2 AIT → ↓ vascularity (destructive thyroiditis). Tx: self-limiting
RAIU: Unreliable due to iodine load from amiodarone
Management: Depends on AIT type and cardiac status (coordinate with cardiology)
⬆️Thyroglobulin=⬆️ endogenous production
39
Multiple Choice
A 48-year-old woman is evaluated for a 6-month history of a 9.1-kg (20.1-lb) weight gain and easy bruising. She has newly diagnosed type 2 diabetes mellitus treated with metformin.
On physical examination, vital signs are normal. BMI is 38. The patient has central obesity, supraclavicular and dorsocervical fat pads, and wide violaceous striae on her abdomen.
Laboratory studies show elevated 24-hour urine free cortisol and late-night salivary cortisol levels.
Which of the following is the most appropriate diagnostic test to perform next?
Abdominal CT
Adrenocorticotropic hormone level measurement
8-mg Dexamethasone suppression test
Inferior petrosal sinus sampling
40
Next test: ACTH level to classify Cushing syndrome
Diagnosis confirmed: ≥2 abnormal tests (↑ urine free cortisol, ↑ late‑night salivary cortisol)
Purpose of ACTH: Distinguish ACTH‑dependent vs ACTH‑independent disease
If ACTH suppressed (<5 pg/mL): ACTH‑independent → adrenal CT/MRI
If ACTH normal/high: ACTH‑dependent → further localization
Not indicated now:
Adrenal imaging (before ACTH result)
High‑dose dexamethasone test (only if ACTH‑dependent, no pituitary lesion)
Inferior petrosal sinus sampling (pre‑surgical confirmation only)

41

42
Multiple Choice
A 72-year-old man is evaluated following surgical fixation of a right distal radius fracture after a fall. Dual-energy x-ray absorptiometry (DEXA) scan performed 2 years ago showed low bone mineral density (BMD). Alendronate weekly was initiated after the scan, and he has been adherent to therapy. Review for secondary causes of osteoporosis is negative. DEXA reassessment shows no significant change in BMD. Which of the following is the most appropriate management?
Add calcium and vitamin D supplementation
Continue alendronate
Order dual-energy x-ray absorptiometry scan of the distal left radius
Measure serum C-telopeptide of type 1 collagen
43
Best management: Continue alendronate
Rationale:
Incident fracture ≠ treatment failure
No significant decline in absolute BMD
Fracture risk reduction not fully reflected by BMD changes
Why not others:
Calcium/Vit D: supplement only if intake deficient
Repeat or distal radius DXA: no meaningful BMD change; high measurement error
Bone turnover markers (eg, C‑telopeptide): unreliable after recent fracture


44
Multiple Choice
A 46-year-old man is evaluated for a thyroid nodule discovered 2 years ago. Thyroid ultrasonography performed at that time showed a 2.5-cm left upper pole isoechoic solid nodule without microcalcification or irregular margin. The sonographic pattern was characterized as low suspicion for malignancy. Fine-needle aspiration biopsy showed benign cytology.
Today, on physical examination, vital signs are normal. A 2.5-cm left upper pole thyroid nodule is firm and mobile. No lymphadenopathy is evident.
Laboratory studies show a normal TSH. Which of the following is the most appropriate next step in management?
Fine-needle aspiration biopsy
Levothyroxine initiation
Thyroid scintigraphy with radioactive iodine uptake
Thyroid ultrasonography
No further evaluation
45
Next step for thyroid nodule: Repeat thyroid ultrasonography
Context: Persistent 2.5‑cm nodule with prior benign FNAB and normal TSH
Rationale:
Benign cytology still carries 2–7% malignancy risk
ATA recommends surveillance US (timing based on sonographic risk)
Why not others:
Repeat FNAB: only if growth or new suspicious features
Levothyroxine: may help to reduce nodule growth, however ↑ risk of thyrotoxicosis
RAIU scan: only for suppressed TSH
No follow‑up: inappropriate due to false‑negative risk

46
Multiple Choice
A 46-year-old woman presents with a 1-year history of A 46-year-old woman presents with a 1-year history of progressive weight‑bearing leg pain and episodic chest pain with prolonged soreness. She has muscle weakness, a waddling gait, weight loss, and postprandial bloating, and takes no medications.
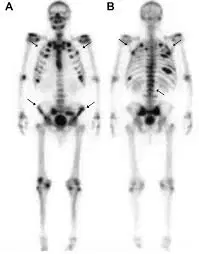
Exam shows bilateral rib tenderness. Labs reveal elevated alkaline phosphatase with low calcium and phosphorus; creatinine is normal. Rib radiograph shows unhealed fractures. Whole-body bone scan shows increased uptake of technetium throughout the skeleton and foci of intense uptake in the ribs and pubic rami bilaterally. Dx?
Bone metastases
Osteomalacia
Osteonecrosis
Osteoporosis
47
Osteomalacia
Diffuse bone pain and skeletal tenderness
Low BMD in setting of malabsorption (eg, celiac disease, gastric bypass)
↑ alkaline phosphatase (early marker)
Supporting labs:
Very low 25‑hydroxyvitamin D
Secondary hyperparathyroidism.
Low urine calcium
Bone scan: Diffuse skeletal uptake + focal hotspots → osteomalacia
Why not others: Metastases: focal uptake, often hypercalcemia
Osteonecrosis: focal, not diffuse
Osteoporosis: does not explain diffuse uptake or biochemical abnormalities
48

XLH: X-Linked Hypophosphatemia
TIO: Tumor-Induced Osteomalacia
49

Endocrinology Board Review
By MS
Show answer
Auto Play
Slide 1 / 49
SLIDE
Similar Resources on Wayground

43 questions
2025 Leadership Development Program - About the Redesign
Presentation
•
Professional Development
44 questions
Unit 4 : part 1 ( Clothes and Colors)
Presentation
•
Professional Development
42 questions
Copy of G4_U5_L12_22-23
Presentation
•
KG - Professional Dev...
44 questions
Introduction to Pedagogy and Teaching Strategies
Presentation
•
Professional Development
44 questions
Apps & applications
Presentation
•
Professional Development
47 questions
Unit 4A Homeostasis & Portfolio
Presentation
•
KG - University
43 questions
Copy of G2_K8_L7_22-23
Presentation
•
KG - Professional Dev...
40 questions
Kingdoms
Presentation
•
KG - University
Popular Resources on Wayground
11 questions
Hallway & Bathroom Expectations
Quiz
•
6th - 8th Grade
10 questions
HCS SCI 03 Summer School Assessment 2
Quiz
•
3rd Grade
11 questions
Home Scope
Quiz
•
7th - 8th Grade
12 questions
2026 TAP Technology in the Classroom
Presentation
•
Professional Development
15 questions
HCS SCI 05 Summer School Assessment 2 Review
Quiz
•
5th Grade
15 questions
HCS SCI 04 Summer School Review 2
Quiz
•
4th Grade
59 questions
Geometry Unit 3 Review
Quiz
•
9th - 12th Grade
14 questions
FAST ELA READING SMAPLE TEST MATERIALS
Passage
•
3rd Grade